
Feeding Tube During Head & Neck Radiotherapy: When, Why & Care Guide
Feeding tubes are very common during head & neck radiotherapy, especially when treatment includes concurrent chemotherapy or covers large mucosal areas (oral cavity/oropharynx/hypopharynx). The goal is simple: prevent weight loss, dehydration, treatment breaks, and aspiration—all of which can worsen outcomes.
Why a feeding tube may be needed during head & neck RT
Radiotherapy can cause:
Severe mucositis (mouth/throat ulcers)
Odynophagia (painful swallowing)
Dysphagia (weak/unsafe swallow)
Thick saliva + loss of taste
- Dry mouth and fatigueThese make it hard to maintain calories and fluids orally.
A tube helps you:
Maintain nutrition + hydration
Take medicines safely
Reduce risk of hospital admission
Avoid treatment interruptions
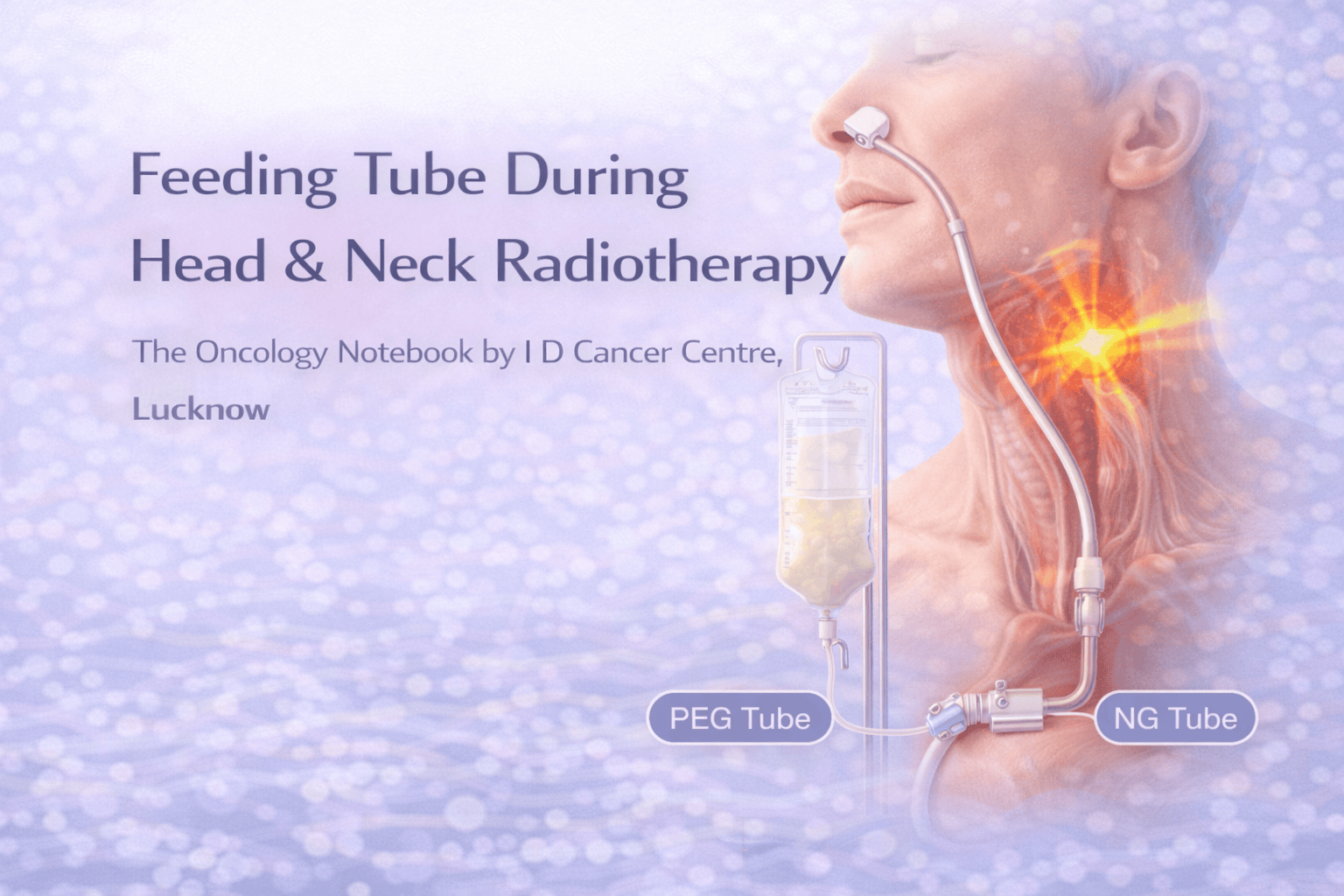
Types of feeding tubes (practical)
1) NG/Ryle’s tube (through nose to stomach)
Usually short-term (days to weeks)
Quick to insert, no procedure room needed in many cases
Can be uncomfortable, may dislodge
2) PEG tube (Percutaneous Endoscopic Gastrostomy)
Usually for longer support (weeks to months)
More comfortable for many patients long-term
Needs an endoscopic procedure
(Some centers also use RIG/PRG—radiology-guided gastrostomy—depending on availability.)
Prophylactic vs reactive tube placement
Prophylactic (planned before RT starts)
Considered when high risk of severe swallowing problems is expected, such as:
Large-field mucosal RT (oropharynx/hypopharynx)
Concurrent chemo-RT
Significant pre-treatment weight loss, poor intake, frailty
Bulky tumors causing dysphagia
Very poor dental/oral condition
Reactive (when problems develop during RT)
Used when a patient starts with good swallowing but later develops:
Inadequate intake for >3–5 days
Weight loss (commonly >5–10%)
Dehydration/IV fluid requirement
Aspiration risk or repeated choking
Key message: needing a tube is not a “failure”—it’s supportive care to help you complete curative treatment safely.
How long does the tube stay?
NG tube: often 1–6 weeks (varies)
- PEG: often 6–12+ weeks depending on recoveryTube removal is considered when the patient can maintain nutrition/hydration orally and swallow is safe.
“Will a tube make my swallowing worse?”
Keep swallowing small sips/soft foods as tolerated (if safe)
Do daily swallow exercises (speech/swallow therapist plan)
Use tube to “top up” nutrition when pain is severe
Practical feeding targets (simple)
During head & neck RT, many patients need:
High calories + high protein
- Frequent small feedsCommon approach: 5–6 feeds/day + water flushes.
Your oncology dietitian will individualize targets, but clinically we watch:
Weight trend
Urine output
electrolytes
treatment tolerance
Tube care essentials (must-know)
Prevent blockage
Flush with water before and after feeds/medicines
Crush medicines only if permitted; use liquid forms when possible
Prevent infection/skin issues (PEG site)
Keep site clean and dry
Watch for redness, discharge, fever, increasing pain
Prevent aspiration
Feed in upright position
Stay upright 30–60 minutes after feed
Stop feeds if coughing/choking worsens
When to call urgently
Fever, chills, PEG-site pus/redness spreading
Tube dislodgement
Persistent vomiting, severe abdominal pain/distension
Inability to flush tube (complete blockage)
Breathing difficulty or repeated choking
