
Dysplasia Explained: What It Means, Cancer Risk, Tests & Treatment (Expert Guide)
“Dysplasia” is one of the most anxiety-provoking words patients see on biopsy or Pap reports. Many people immediately think it means cancer. It doesn’t. Dysplasia means abnormal (pre-cancer) cell changes—a stage where doctors can intervene to prevent cancer.
Dysplasia can occur in different tissues such as the cervix, mouth, throat, colon, skin, and elsewhere. The exact risk depends on where it is, how severe it is, and whether the cause continues (like tobacco/areca nut, HPV, chronic inflammation).
This expert guide explains dysplasia in simple terms, how it’s graded, what “mild/moderate/severe” means, what tests confirm it, and what treatment and follow-up usually look like.
1) What is dysplasia?
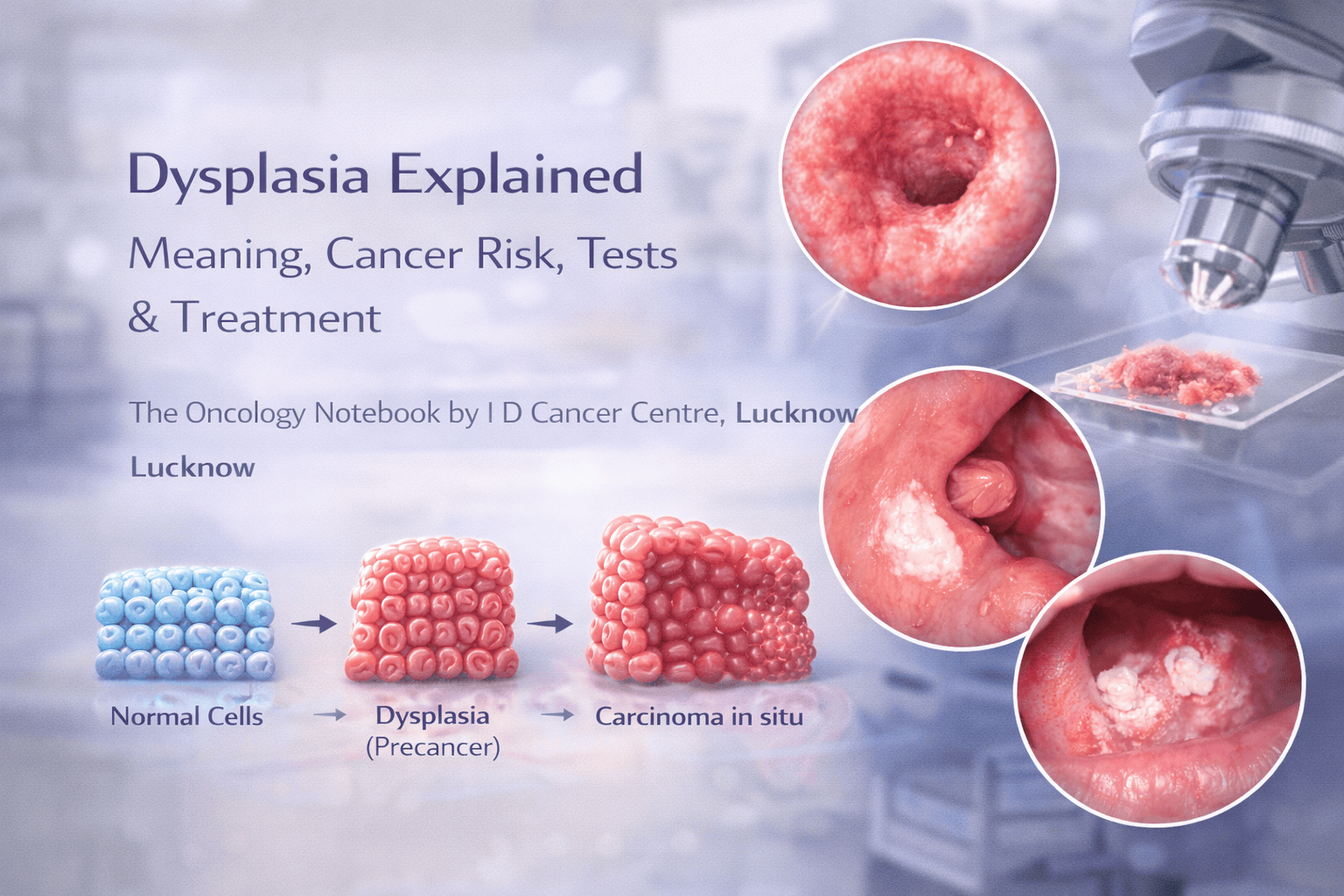
Think of it as a warning sign on a spectrum:
Normal cells → irritation/inflammation → dysplasia (pre-cancer) → carcinoma in situ → invasive cancer
Not all dysplasia progresses to cancer, especially if the cause is removed and proper treatment/follow-up is done.
2) Dysplasia vs cancer: the key difference
Dysplasia: abnormal cells are confined to the surface lining; no invasion into deeper tissues.
Invasive cancer: abnormal cells break through the basement membrane and invade deeper tissues; can spread.
That’s why dysplasia is often called “precancer”—a stage where cancer can still be prevented.
3) Why dysplasia happens (common causes)
Dysplasia usually develops due to ongoing injury or infection that repeatedly damages cells.
Common causes (India-relevant)
Tobacco chewing and smoking
Areca nut (supari/gutkha/pan masala) → associated with OSMF and oral dysplasia
Alcohol (especially with tobacco)
HPV infection (most important for cervical dysplasia and some throat lesions)
Chronic inflammation/irritation (e.g., reflux in esophagus, chronic ulcers, certain colitis conditions)
Often, removing the cause significantly reduces risk and can allow low-grade changes to regress.
4) Where dysplasia is commonly seen (patient examples)
A) Cervix (Pap/HPV pathway)
Dysplasia here is commonly called CIN (Cervical Intraepithelial Neoplasia).
Often linked to high-risk HPV.
B) Mouth (oral cavity)
Dysplasia may be found in leukoplakia (white patch), erythroplakia (red patch), OSMF, or chronic ulcers.
Strongly linked to tobacco/areca nut.
C) Colon
Found in polyps; removal prevents colon cancer.
D) Esophagus
Barrett’s esophagus can develop dysplasia due to chronic reflux.
Each site has different management strategies, so the biopsy report location is crucial.
5) Grading of dysplasia: mild, moderate, severe
Pathology grading reflects how abnormal the cells look and how much of the lining is involved.
Low-grade dysplasia (mild)
Early changes
Lower risk of progression
Often managed with cause removal + observation or local treatment depending on site
High-grade dysplasia (moderate to severe, depending on system)
More significant changes
Higher risk of progression
Often requires active treatment (excision/ablation) and close follow-up
Carcinoma in situ
Very advanced pre-cancer (full thickness abnormality in lining)
Still non-invasive but treated aggressively like “very high-grade dysplasia”
Important: Different organs use different terminology:
Cervix: CIN1 (low grade), CIN2/3 (high grade)
Cervical cytology: LSIL/HSIL
- Oral cavity: mild/moderate/severe epithelial dysplasiaYour doctor interprets it for your site.
6) Does dysplasia always turn into cancer?
No. Dysplasia can:
Regress (especially low grade if cause is removed)
Stay stable
Progress (risk increases with high grade and ongoing exposure)
Factors that increase progression risk
High-grade dysplasia
Persistent high-risk HPV (cervix)
Continued tobacco/areca nut use (mouth)
Large lesions or lesions in high-risk areas (e.g., floor of mouth, side of tongue)
Immunosuppression (HIV, transplant meds)
Poor follow-up
7) How is dysplasia diagnosed?
Dysplasia is not diagnosed reliably by symptoms alone. It is confirmed by testing.
A) Biopsy (gold standard)
A biopsy shows the grade of dysplasia and rules out invasive cancer.
B) Site-specific tests
Cervix: Pap test, HPV test → colposcopy → biopsy
Mouth: clinical exam → biopsy from suspicious areas
Colon: colonoscopy → polyp biopsy/removal
Esophagus: endoscopy → biopsy
Key rule: If a doctor suspects dysplasia, biopsy is the definitive step.
8) Symptoms: can dysplasia cause symptoms?
Often, dysplasia causes no symptoms. When symptoms occur, they are usually due to the underlying lesion.
Oral dysplasia
Persistent white/red patch
Mild burning, roughness
Non-healing ulcer
Cervical dysplasia
Usually asymptomatic
Detected by screening (Pap/HPV)
Bleeding after sex is more concerning for cervical pathology and needs evaluation
So, screening and examinations matter.
9) Treatment: what happens after a dysplasia diagnosis?
Management depends on site + grade + patient factors.
General principles
Confirm no invasive cancer (adequate biopsy)
Remove the cause (stop tobacco/areca, treat HPV-related lesions, treat reflux, etc.)
Treat the lesion if high risk
Follow-up regularly (because recurrence can happen)
10) Treatment by common site (practical overview)
A) Cervical dysplasia (CIN/HSIL)
Low-grade lesions may be observed in some cases
High-grade lesions often need treatment such as excisional procedures (e.g., LEEP/conization) depending on clinician plan
Follow-up Pap/HPV schedules are critical
B) Oral epithelial dysplasia
Habit cessation is mandatory (tobacco/areca)
Low-grade: may be monitored or removed depending on lesion features
High-grade: often treated with excision/laser in appropriate settings
Regular oral screening is essential
C) Colon dysplasia in polyps
Polyp removal often prevents progression
Surveillance colonoscopy intervals depend on pathology
D) Barrett’s dysplasia
Reflux control + endoscopic therapies in selected cases
Close surveillance
Your team will tailor a site-specific plan.
11) Follow-up: why it’s non-negotiable
Even after treatment, dysplasia can recur or new lesions can develop—especially if the exposure continues.
Follow-up typically includes:
Clinical exam at planned intervals
Repeat Pap/HPV or repeat biopsy if changes occur
Imaging is not usually needed for dysplasia unless cancer is suspected
If you stop the cause and follow the plan, outcomes are usually excellent.
12) “Red flags” that need urgent reassessment
Regardless of prior dysplasia diagnosis, seek urgent evaluation if you develop:
Rapidly enlarging lesion or thickening
Non-healing ulcer > 2 weeks
Bleeding from lesion
New neck lump
Unexplained weight loss
Worsening pain or difficulty swallowing
These could indicate progression or a separate process.
13) Frequently asked questions
Is dysplasia the same as “precancer”?
Yes—dysplasia is commonly a precancer change, but risk varies by grade and site.
Can dysplasia go away?
Low-grade dysplasia can regress, especially if the cause is removed and the immune system clears infection (e.g., HPV). High-grade usually needs active treatment.
Should I repeat biopsy?
Repeat biopsy is advised if:
The lesion changes
Symptoms worsen
The initial biopsy was small/inadequate
Doctor suspects higher-grade changes
What lifestyle changes help the most?
Stop tobacco, supari/gutkha/pan masala completely
Limit alcohol
Improve oral hygiene and nutrition
Follow screening schedules (Pap/HPV)
Manage reflux if relevant
Key takeaways (expert summary)
Dysplasia means pre-cancer cell changes, not cancer.
Risk depends on grade (low vs high) and the site.
Biopsy confirms dysplasia and rules out invasive cancer.
Stopping the cause (tobacco/areca/HPV risk management) + correct treatment + follow-up prevents progression.
High-grade dysplasia needs prompt treatment and close monitoring.
Get guidance at I D Cancer Centre
If you have a biopsy report showing dysplasia (mouth/cervix/other), persistent white/red patch, non-healing ulcer, or abnormal Pap/HPV report, we can guide next steps, staging (if needed), and prevention-focused care.
